


Healthcare
OSHAid is the mobile app that simplifies hazard assessments for healthcare workplaces.
Pre-loaded with the hazards specific to healthcare (patient handling and ergonomic injuries, slips and falls, bloodborne pathogen exposure and infectious disease risk, sharps and needlestick injuries, hazardous drug and disinfectant exposure, radiation in imaging units, stress and psychosocial risk, night-shift fatigue, hallway co-activity, and regulated medical waste handling), OSHAid guides you step by step to identify, evaluate, and prevent everyday hazards.
Result: an always-up-to-date hazard assessment, less paperwork, and audit-ready OSHA compliance.


Beta version
Free download

OSHAid

Built for healthcare
OSHAid for healthcare is built on proven sector expertise. The app comes pre-loaded with the main hazards specific to your operation (such as bloodborne pathogen exposure, sharps and needlestick injuries, patient handling and ergonomic strain, slips on wet floors, hazardous drug and disinfectant exposure, infectious disease risk, and workplace violence) along with recommended prevention measures aligned with OSHA standards.
You can complete this information at any time by adding your own hazards and adjusting them in real time directly from your mobile device.
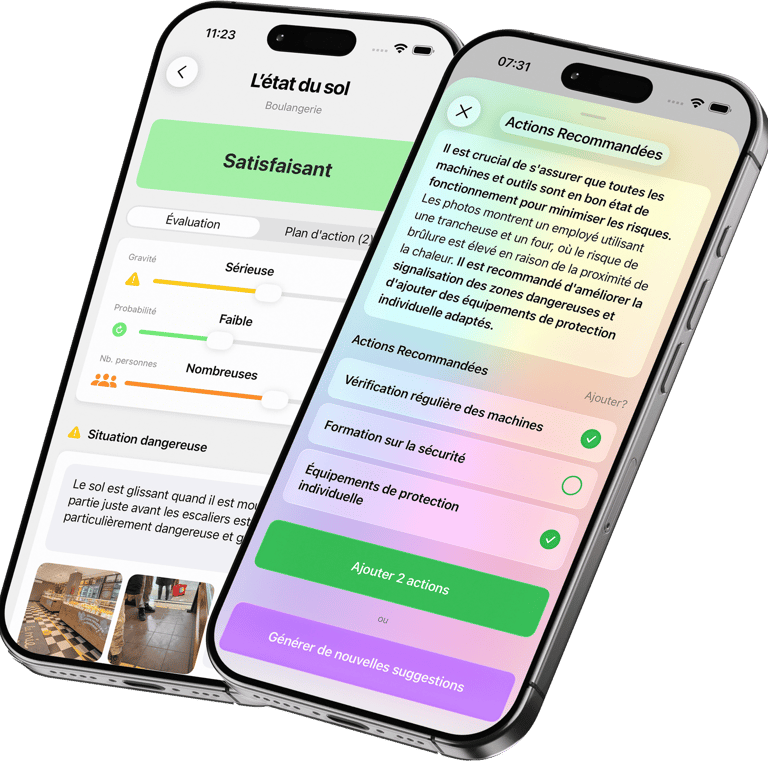
Thanks to its step-by-step guidance, OSHAid helps you assess, prioritize, and document hazards quickly, while significantly reducing exposure for your clinical and support teams.


Pre-loaded equipment list
OSHAid lets you add your most-used equipment to one centralized list. Each product card details the associated hazards, safety guidelines and best practices to protect your employees when operating the equipment.
All documentation can be updated remotely: you always have the latest recommendations on hand, along with manufacturer contacts for maintenance and support.
Real-time updates for every user, simultaneously
Accessible anywhere, anytime, from your mobile device
Customizable and interactive: add your own equipment or adapt the guidelines to match your day-to-day reality
The result: better information and stronger safety.


Benefit from the community's experience
OSHAid draws on the collective experience of its entire user base to continuously enrich and update its recommendations. Every update strengthens safety for every user. Tap into the strength of the community to anticipate hazards and durably reduce your exposure.

Customer story
OSHAid is built for the day-to-day reality of a healthcare facility manager. In just a few minutes, I can add the areas and equipment that really matter to us (rooms, treatment rooms, OR, pharmacy, linen, carts, patient lifts, infusion devices, biohazard waste, disinfection products...). Each card is clear: hazards, guidelines, best practices, and above all the simple actions to put in place. The result: teams have the right reflexes, even during peak activity, and we avoid the "small oversights" that sometimes turn into incidents (falls, MSDs, blood/body-fluid exposure, chemical exposure). The real bonus: everything updates remotely. I always keep the latest recommendations, and I can adjust our guidelines to fit the organization (new protocol, new equipment, redesign of a unit) without starting from scratch or chasing binders. The bottom line: we save time, the team is better informed, and prevention becomes a natural part of daily life — with real peace of mind in case of an inspection or audit. — Claire Dumas, Healthcare Facility Director (Lyon)


OSHA FAQ for Healthcare
What is an OSHA hazard assessment in healthcare?
A healthcare hazard assessment is a structured review that identifies, evaluates, and prioritizes the workplace hazards employees may be exposed to in a hospital, clinic, dental office, urgent care, lab, ambulatory surgery center, long-term care facility, behavioral health setting, or home-care service. In healthcare, the assessment converts what is observed at the bedside, in the OR, in the lab, and on the ward into specific prevention actions that protect staff, patients, and visitors.
Does OSHA apply to healthcare facilities?
Yes. OSHA applies to almost every private-sector healthcare employer in the U.S. — hospitals, physician and dental practices, nursing homes, dialysis centers, surgery centers, behavioral health facilities, pharmacies, labs, and home-health agencies. Several federal OSHA standards target healthcare specifically, including 29 CFR 1910.1030 (Bloodborne Pathogens), the Needlestick Safety and Prevention Act, 29 CFR 1910.1200 (HazCom for hazardous drugs and disinfectants), and the General Duty Clause for workplace violence in healthcare.
Does a small clinic or dental office with only one employee need an OSHA program?
Yes. As soon as a healthcare practice hires one employee — a medical assistant, dental hygienist, RN, LPN, tech, sterile-processing aide, or front-desk staff — the practice becomes an OSHA-covered employer and must run a written safety program for the standards that apply to its work.
Why is hazard assessment so important in healthcare?
Healthcare workers face a uniquely broad mix of hazards: bloodborne pathogen exposure, sharps injuries, infectious disease, hazardous drugs, slips and falls, patient handling injuries, workplace violence, ionizing radiation, and shift-work fatigue. A current hazard assessment is the foundation of a written exposure control plan, employee training, PPE selection, and engineering controls.
What are the main hazards an OSHA program for healthcare must address?
A healthcare safety program should cover bloodborne pathogens (BBP) and other potentially infectious materials, needlestick and sharps injuries, hazardous drugs (USP <800>), disinfectants and sterilants (e.g., glutaraldehyde, peracetic acid), tuberculosis and respiratory pathogens, ionizing and laser radiation, ergonomics and safe patient handling, slips and trips, latex sensitization, workplace violence, and psychosocial stress.
What clinical-area hazards must be evaluated?
Clinical areas need targeted evaluations for sharps and BBP exposure, blood and body fluid splash, contact with contagious patients, sterile processing chemical exposure, fit-tested respiratory protection (29 CFR 1910.134) for TB and airborne diseases, ergonomic strain from repetitive motion and patient handling, prolonged standing, surge and emergency-response pressure, and tense interactions with patients or families.
Which healthcare roles are covered by OSHA?
Every role with at least one employee is covered — physicians, dentists, RNs, LPNs, CNAs, NAs, medical and dental assistants, techs, pharmacists and pharmacy techs, lab staff, sterile-processing techs, environmental services, transport, dietary, security, administrative staff, and clinical leadership in inpatient, outpatient, and home-care settings.
Which "work units" should the OSHA hazard assessment cover?
The assessment should mirror how the facility actually operates: reception/check-in, triage, exam and treatment rooms, the OR, sterile processing/CSSD, pharmacy, lab, imaging, patient rooms, ICU, ED, behavioral health units, home visits, housekeeping/EVS, linen and waste handling, transport, kitchen and dietary, supply and dock, and administrative areas.
How do you build an OSHA-compliant healthcare safety program?
Start by mapping the work units, identifying hazards in each (chemical, biological, ergonomic, physical, psychosocial, and workplace violence), and analyzing actual exposure scenarios. Apply the Hierarchy of Controls, write the required programs (BBP, HazCom, Respiratory Protection, Workplace Violence, Sharps Injury Log, etc.), train staff in a language they understand, and document everything. A strong healthcare program is practical, role-specific, and built on what actually happens at the bedside.
When should you update a healthcare safety program?
Update it any time the work or its hazards change — a new clinical service line, a new hazardous drug or disinfectant, a new piece of equipment, a unit reorganization, a new exposure pathway, a sharps injury, a workplace violence event, or a near miss. OSHA expects programs to track real conditions, not stay frozen on a binder.
What documents and inputs help build a healthcare safety program?
Use OSHA Forms 300, 300A, and 301; the facility's BBP exposure incident log; sharps injury log; SDS for every chemical and hazardous drug; equipment manuals; infection-control protocols; respirator fit-test records; behavioral-event reports; staffing schedules; and direct conversations with the people doing the work. The closer the program reflects reality, the more useful it is.
Is there an OSHA template for clinics, hospitals, dental offices, or pharmacies?
OSHA publishes free model exposure control plans (notably for BBP), eTools, and small business resources at osha.gov. The OSHA On-Site Consultation Program will help small healthcare employers build a compliant program at no cost. A template is only a starting point — the program must be tailored to your services, equipment, patients, and workflows.
What's the difference between a generic safety program and one built for healthcare?
A generic plan stays theoretical. A healthcare-specific program names the real exposures: BBP and sharps, hazardous drug compounding, sterile processing chemistry, contagious disease screening, ergonomic patient handling, workplace violence in the ED and behavioral health, and the pace of clinical work. In healthcare, an overly generic document quickly fails the inspection and the staff.
Can a strong OSHA program improve safety in a clinic or hospital?
Yes. Facilities that operate active Safety and Health Programs see fewer needlesticks, fewer lifting injuries, fewer workplace violence events, lower workers' comp costs, and stronger employee retention. The program becomes a tool to drive prevention, prioritize investment, train teams, and strengthen the safety culture.
What are the most common OSHA-recordable injuries in healthcare?
The most common are needlestick and sharps injuries, exposures to blood and body fluids, patient-handling musculoskeletal injuries, slips and falls on wet floors, contact dermatitis from gloves and disinfectants, exposure to hazardous drugs, workplace violence injuries (especially in EDs and behavioral health), and stress-related conditions.
Long-term care, home health, dental, pharmacy, lab — do safety programs need to be different by setting?
Yes. Each setting has its own dominant hazards. Long-term care emphasizes patient handling, falls, and dementia-related violence. Home health emphasizes solo-worker safety, driving, and unknown-environment exposures. Dental focuses on aerosols, sharps, and amalgam handling. Pharmacy and labs focus on hazardous drugs and chemical safety. Each program must be tailored to that real activity.
Does the program need to address workplace violence and psychosocial hazards?
Yes. Workplace violence in healthcare is one of the most serious hazards OSHA addresses under the General Duty Clause; OSHA's voluntary Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers are the primary federal reference. Programs should also address staffing pressure, fatigue, surge events, and high-acuity stress — each can directly affect employee safety and care quality.
Is an OSHA program useful beyond compliance for a hospital or clinic?
Yes. A well-built program is a leadership tool, not just paperwork. It surfaces priorities, tracks corrective actions, organizes training, reduces injuries, lowers turnover, and protects the facility from costly citations. In healthcare, it becomes a true operational management tool that supports both worker safety and patient care.
Simple, fast, and effective
Try OSHAid for free, no commitment.

Solutions for large organizations
Beta version

Free download
